Dr. Rudzki had the privilege of training in Sports Medicine and developing his knee surgical skills at Washington University in St. Louis and the Hospital for Special Surgery in New York City. He has performed high-caliber research on cartilage transplantation as well as ACL injury in NHL players and written articles on bioabsorbable knee implants and fracture fixation about the knee.
Dr. Rudzki has a high level of expertise in the performance of arthroscopic ligament reconstruction, cartilage restoration, complex meniscal repair, treatment of patellar instability, osteotomy and fracture treatment about the knee in a wide range of athletes from adolescents to professionals. He serves on the clinical faculty of the George Washington University School of Medicine teaching medical students and orthopaedic surgical residents. As a consultant for Arthrex and Stryker, Dr. Rudzki engages heavily in medical education to train surgeons and product specialists on emerging techniques and engages with engineers on product design teams to help develop better tools and techniques. As a member of the AAOS Evaluation Committee, he spent several years writing questions on knee injuries and surgical treatments for surgeons in practice and in training.
Meniscal Tears & their Treatment: The menisci are C-shaped shock-absorbing semi-circular rings of Type 1 Fibrocartilage that serve to protect the Type 2 hyaline articular cartilage that covers the ends of the femur and tibia. The coefficient of friction of articular cartilage is approximately 1/5 to 1/7 that of ice sliding on ice. With time, sports activities, life and age our cartilage gradually accumulates injury and begins to deteriorate. The menisci play a critical role in preserving the structure and function of the articular cartilage in our knees. Meniscal tears are typically incapable of healing because they have a poor blood supply which comes in from the periphery and an avascular zone in the central third.
Meniscal Tears and meniscal surgery is often misunderstood and mischaracterized. Traumatic tears in young individuals will not heal and can be a source of persistent pain, mechanical symptoms, swelling and dysfunction. With time, life, and age the prevalence of meniscal tears increases and therefore they become an increasingly more common finding over age 45-50. If they are asymptomatic, they are an incidental finding best left alone. If they are responsible for pain and mechanical symptoms, then oral anti-inflammatories, ice, activity modification and physical therapy are the preferred conservative treatment.
For traumatic tears in young athletes or persistently symptomatic tears that fail to respond to conservative treatment, surgical intervention is appropriate and can be of significant benefit to patients. A great deal of research from the work of Drs. Russell Warren and Stephen Arnoczky at Hospital for Special Surgery to that of Dr. Ashesh Bedi of the University of Michigan has helped us to better understand the indications for when these tears should be repaired and when the irreparable meniscal tissue should be resected. Of key importance in understanding these surgeries, is the principle that only torn/irreparable/dysfunctional tissue is removed and only when appropriately indicated.
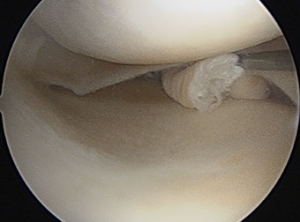
The following is case example of a bucket-handle meniscal tear with a rare opportunity for a second-look to confirm healing at the time of a staged ACL reconstruction in a young female athlete.
Related Posts
Elite Sports Medicine Care from High School to College
Posted on: 10-Nov-2021
Our team first met Matt after a lacrosse-related knee injury in which he tore his ACL and had a severe meniscus injury called a “bucket-handle” tear. Through a staged pair of surgeries, his meniscus was
Chief Complaint/Injury Jeff is a hiker, skier, and fitness enthusiast who suffered an acute injury to his left knee due to a skiing accident in March of 2017. He came to us with an unstable
Patient Testimonial: Hiking and skiing after ACL reconstruction and ACL Rehab
Posted on: 14-May-2018
ACL REHAB: Skiing, Hiking, Martial Arts, & Patient Goals Many patients want to get back to skiing after ACL rehab. From adolescent racers to helicopter skiers in the back-country and recreational skiers in their