Dr. Rudzki had the privilege of training in Sports Medicine and developing his knee surgical skills at Washington University in St. Louis and the Hospital for Special Surgery in New York City. He has performed high-caliber research on cartilage transplantation as well as ACL injury in NHL players and written articles on bioabsorbable knee implants and fracture fixation about the knee.
Dr. Rudzki has a high level of expertise in the performance of arthroscopic ligament reconstruction, cartilage restoration, complex meniscal repair, treatment of patellar instability, osteotomy and fracture treatment about the knee in a wide range of athletes from adolescents to professionals. He serves on the clinical faculty of the George Washington University School of Medicine teaching medical students and orthopaedic surgical residents. As a consultant for Arthrex and Stryker, Dr. Rudzki engages heavily in medical education to train surgeons and product specialists on emerging techniques and engages with engineers on product design teams to help develop better tools and techniques. As a member of the AAOS Evaluation Committee, he spent several years writing questions on knee injuries and surgical treatments for surgeons in practice and in training.
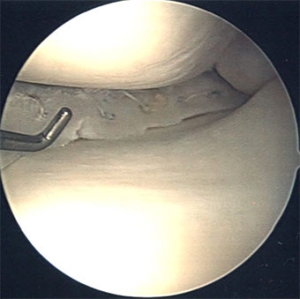
25 year-old female with prior ACL injury treated conservatively and new onset functional instability resulting in bucket-handle medial meniscal tear with loss of both flexion and extension. In ideal cases, particularly in young patients, these tears are treated with arthroscopic medial meniscal repair.
We discussed the risks and benefits of a staged approach. Given her loss of flexion and extension, a combined repair of her bucket-handle medial meniscal tear and ACL reconstruction would have an unacceptably high risk of arthrofibrosis (stiffness after surgery that can be a serious condition requiring additional procedures and compromised outcome). As a result, we decided to proceed with an acute arthroscopic inside-out repair of her bucket-handle medial meniscal tear followed by a course of rehabilitation and subsequent ACL reconstruction with hamstring autograft.
The outpatient procedure is performed with a combined regional and lighter general anesthetic. The tear is reduced (placed back into position) and multiple sutures placed with a suture passing device through the meniscus and capsule. An incision is made on the medial or lateral side of the knee to carefully dissect down to the capsule, retrieve the needles and tie knots to complete the repair. We often incorporate a notch-pasty and microfracture which facilitates meniscal healing through recruitment of additional bleeding with stem cells and an enhanced healing response.
Meniscal tears are incredibly common and can be a source of not only pain and mechanical symptoms, but progressive degeneration of the knee. The fibrocartilage rings serve as shock-absorbing protectors of the hyaline articular cartilage which lines the tip of the femur and the top of the tibia. Physical therapy can often be successful in the treatment of degenerative meniscal tears. Acute traumatic tears in younger athletes such as the example shown in this case study typically require surgical intervention.
Dr. Rudzki uses several different arthroscopic techniques to treat meniscal tears including an all-inside approach demonstrated in this video:
This brief presentation summarizes the fundamental principles of meniscal tear treatment. Tears are categorized as:
acute vs degenerative
location (relevant for blood supply and healing)
type (radial, horizontal, vertical, parrot-beak, bucket-handle)
potential reparability (very difficult to ascertain from MRI)
Related Posts
Elite Sports Medicine Care from High School to College
Posted on: 10-Nov-2021
Our team first met Matt after a lacrosse-related knee injury in which he tore his ACL and had a severe meniscus injury called a “bucket-handle” tear. Through a staged pair of surgeries, his meniscus was
Chief Complaint/Injury Jeff is a hiker, skier, and fitness enthusiast who suffered an acute injury to his left knee due to a skiing accident in March of 2017. He came to us with an unstable
Patient Testimonial: Hiking and skiing after ACL reconstruction and ACL Rehab
Posted on: 14-May-2018
ACL REHAB: Skiing, Hiking, Martial Arts, & Patient Goals Many patients want to get back to skiing after ACL rehab. From adolescent racers to helicopter skiers in the back-country and recreational skiers in their